In 1932 the famous US Supreme Court Justice, Louis Brandeis, wanted to highlight one of the amazingly important, but often overlooked, aspects of the governmental structure of the United States: the tripartite separation of “rights and power” between the People, who start with all the rights and all the power according to the Preamble of the Constitution, and the Federal Government, which is only supposed to be granted the power that is written down, enumerated, in the Constitution, and the States, which is the default place for powers not specifically granted to the Feds on the one hand and specifically granted by the People through their state legislative bodies.
What did Judge Brandeis say?
Source: Library of Congress
“A single courageous State may, if its citizens choose, serve as a laboratory; and try novel social and economic experiments without risk to the rest of the country.“
What does this have to do with COVID-19 you ask?
The experiment of NOT sheltering-in-place and shutting down businesses.
It turns out that seven states did not shut down businesses for the COVID-19 pandemic while 43 states did. [To be clear however, schools were shut down in 49 of 50 states. This despite the known facts that COVID-19 in children is either mild or asymptomatic and deaths are much lower than for influenza.]
So in seven states, lives were disrupted because childcare instead of school was a new necessity for people with children to deal with but nothing else changed. No businesses were closed, no restaurants shuttered, churches were unaffected, etc. If political science was a science it would frame this situation as a hypothesis; to wit:
Based on our understanding of COVID-19 infectivity, we hypothesize that the states that did not restrict its citizen’s movements would have either a higher rate of infection (cases per week or month) or a higher number of infections (total cases cumulatively) or both.
The Figure below is taken from the excellent COVID-19 website maintained by Johns Hopkins which can be found here: Daily cases per 100,000 citizens from Jan 1 to Jun 9
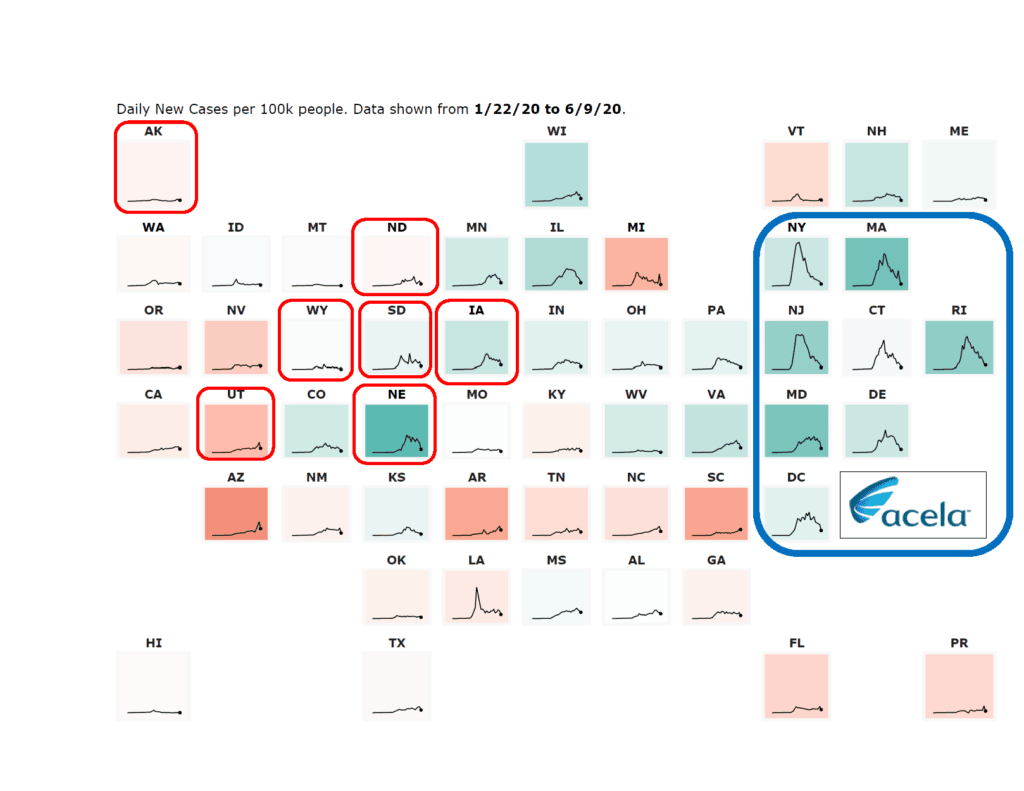
For orientation what you are looking at are the individual states with their two letter abbreviation, a squiggly line for the three day moving average number of cases per 100,000 population and a color code of green, where cases are going down and red where cases are going up. I am purposely not going down into the weeds in each state because we are looking for BIG signals which should be visible at this level of looking at all the states as a group. For now, please ignore all those states in the big blue box.
The seven states with the red boxes around them are the seven states that did not lock their citizens at home. What jumps out at you about these seven states when you compare them to the other states is…nothing! What I mean is that they look pretty interchangeable with the states that completely shut down. Nebraska seems to have the biggest cumulative cases but it looks a lot like Minnesota, Illinois, and Michigan in total area under the curve. As you are well aware, those states really restricted their citizens.
So based on this data, you would have to conclude that your hypothesis is proven to be wrong.
Could the lack of cases in these states be due to factors like population density, lack of large public transportation systems (see below), or any one of a number of other factors. Sure, and if I was in a university we could sit around and have lively facility lounge debates on this for months. But if you are making public policy decisions that are weighing shutting down a state’s economy for months you should be absolutely sure of your facts because your actions effect millions of lives and livelihoods. This was a colossal mistake.
Should SARS-CoV-2 be renamed the ‘Acela Virus?’
Now let’s focus on the blue box. When I was studying this chart without the blue box which I put there I was puzzled about some of the state results. For example: New York and California have very similar demographics, big cities, etc. yet their COVID-19 cases on a population basis could not be different. One obvious difference is that Californians get around in their cars while New Yorkers us a lot of public transportation.
But other unexpected states jumped out. For example, what’s with Rhode Island seeming to be almost as bad as New Jersey? I love Rhode Island but it doesn’t have the ‘feel’ of New York or New Jersey for me, at least. And Delaware, the same question comes up.
And then it hit me, what is the Acela Train Route and which states does it go through?
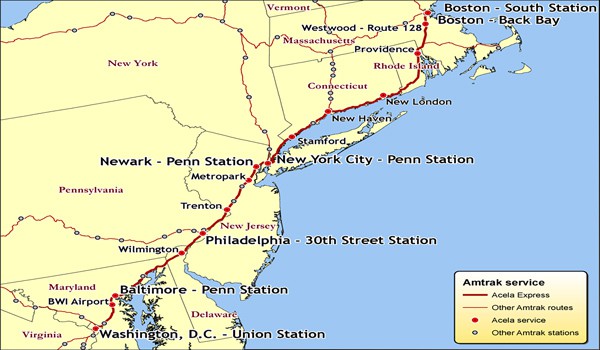
Source: Acela Route
Suddenly this corner of high COVID-19 incidence states made complete sense.
To help you see what I mean I have put a box around the states that the Acela train goes through (it includes Washington, DC). With this as an organizing principle it all comes together. This daily train service from Boston to Baltimore carried about 9600 passengers per day in 2016.1 If COVID-19 was in the US in January2 as some at the CDC think or even the end of December, as I published with a distinguished UCLA statistician before the CDC report in a blog,3 it would have been spreading for about two months until the Acela was closed, initially between New York and Washington on March 7th, and finally completely closed on March 23rd. That is close to 600,000 people in close contact inside a train for the first two months of COVID-19 spread in the US. I did go deep into each state and the peak you see is about 10 to 14 days after the Acela was closed.
Final thought. I know the virus doesn’t have a brain but if it did, and if its mission was to hit hardest all of the people in government, the media, and key academic centers that make decisions that affect the entire country, the entire United States, the Acela train would be the exact place it would want to go.
Suddenly what might look like an over-reaction (from the middle of the country) by the Federal government, the media, and even our academic centers looks more like a very human response to everyone having their riding buddy or friend, the folks they go back and forth with daily, getting COVID-19 or knowing someone with the virus.
If that was happening to you and when you got to the office you were pulling the levers of power all day…well you see where this ends up. Please start a new trend in social media by sending this blog to your friends with the hashtag #AcelaVirus